Skull Fractures can be divided into 2 groups:
- Skull Vault
- Base of Skull
SKULL VAULT
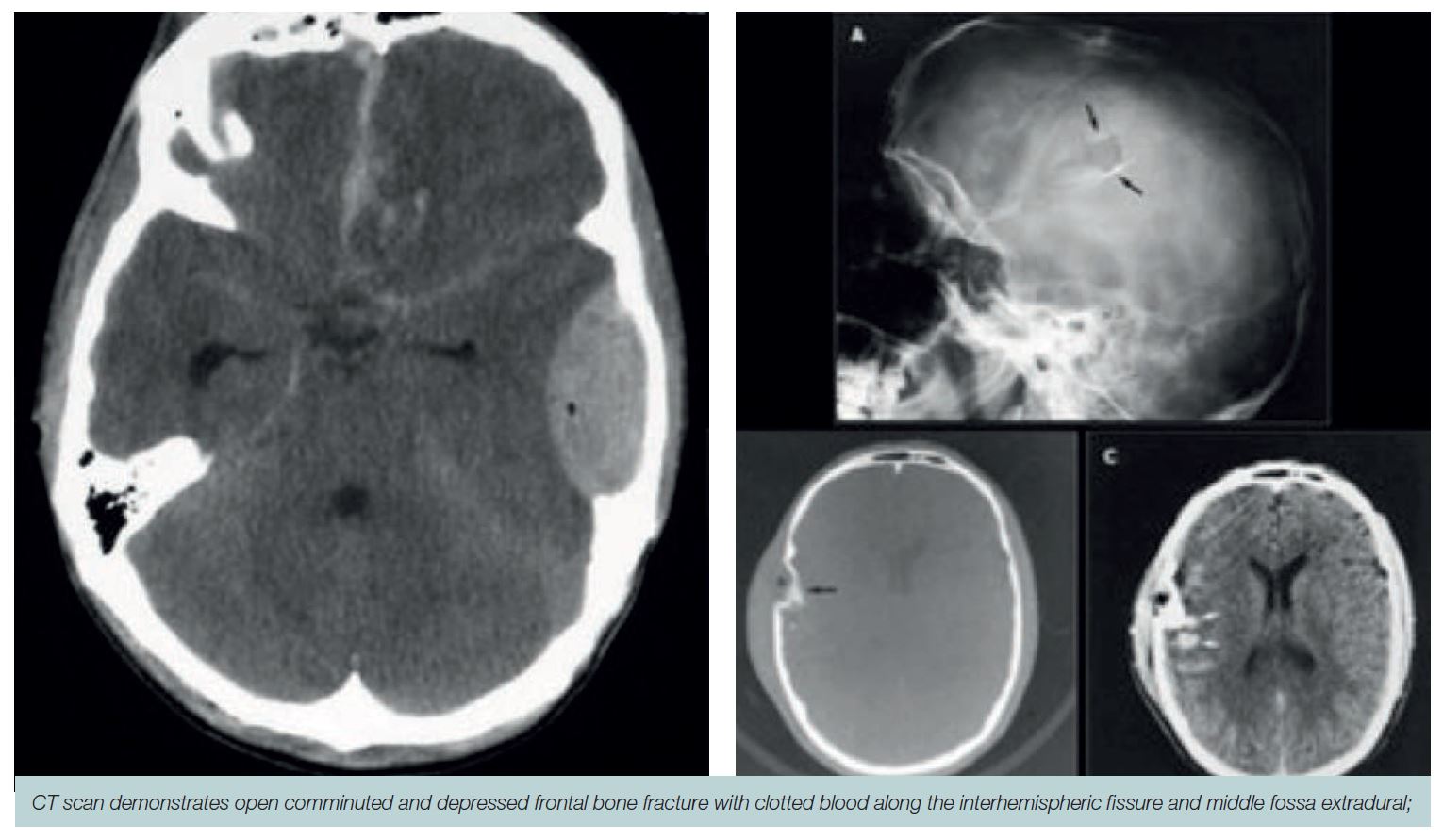
These may be closed or open (compound depressed or depressed, and if depressed it may or may not be a dural laceration underlying contusion).
Clinical
- Soft tissue swelling overlying the involved area
- Laceration with palpable depression below
Investigations
- CT Scan with bone windows and fine slices through the suspected area is the gold standard. Plain skull X-rays may or may not show evidence of a fracture
- MRI may or may not show a fracture but is more important in showing whether or not there is damage to the underlying parenchyma, and potentially a dural laceration
Management
- Closed not displaced skull fractures are treated conservatively
- Open skull fractures: The wound should be debrided, thoroughly cleaned and sutured. If there is evidence of depression (the outer table has gone beyond the inner table) then elevation is indicated
- Evidence of dural laceration and underlying contusion, increases the risk of intracranial infection and seizures. Surgery is more likely to be performed in these cases although elevation of the depressed fracture if there has been a dural laceration and contusion does not necessarily decrease the risk of epilepsy
- “Cosmetic” elevation: in the case of a closed fracture, where the outer table has gone beyond the inner table, then elevation needs to be seriously considered. In an open depressed fracture, elevation is usually performed on lesser depressions
- Antibiotics usually not given for a closed fracture. More likely in open fracture
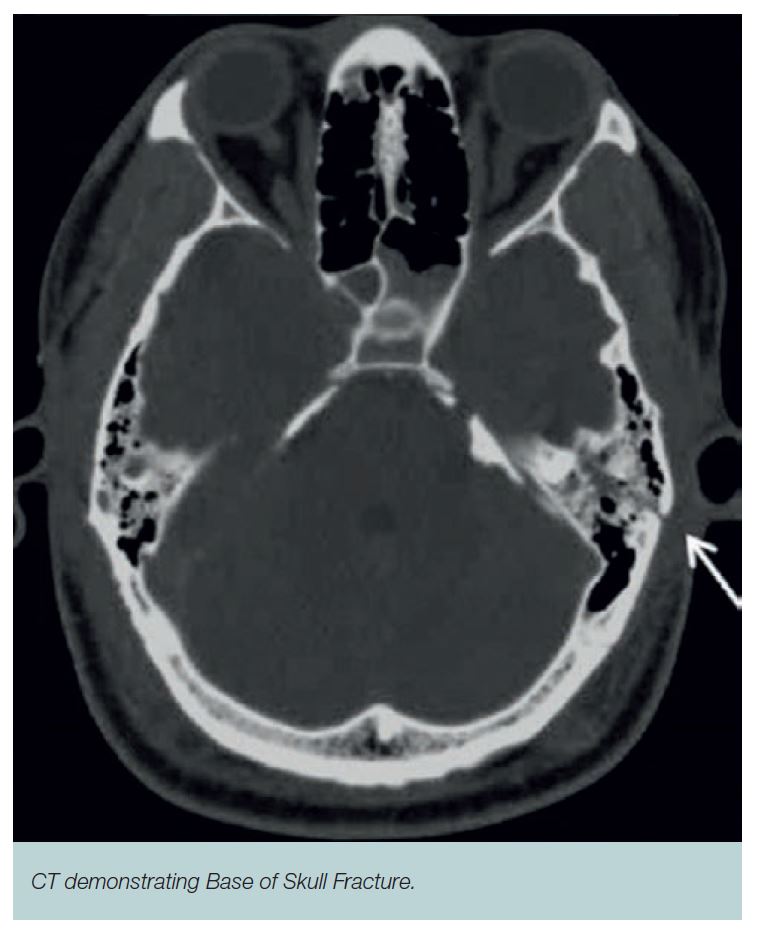
FRACTURED BASE OF SKULL
In order to cause a fractured base of skull a patient needs to suffer a significant injury to the skull. This may be a difficult diagnosis both clinically and radiologically.
Clinical
- CSF Rhinorrhoea
- CSF Otorrhoea
- Bilateral periorbital bruising (raccoon eyes, usually associated with periorbital nasal fractures)
- Mastoid bruising, also known as battle signs, whether it’s bruising behind the ear of the mastoid process
- Anosmia due to fractures through the ethmoid sinuses
- Hemotympanum: Blood in the external auditory canal where there does not appear to be any injury to the external structures of the ear
Investigations
- CT Scan with bone windows and fine slices through the suspected area is the gold standard
- Plain skull X-rays may or may not show evidence of a fracture
- MRI may or may not show a fracture but is more important in showing whether or not there is damage to the underlying parenchyma (not as common as with depressed skull fractures)
- Biochemical, Beta2 transferrin can be used to see if CSF is present
Management
Most base of skull fractures do not require any surgical intervention unless there is evidence of CSF, rhinorrhoea or otorrhoea which does not settle.
- Antibiotics are not indicated
- Discussion with a Neurosurgeon and possible transfer is always recommended.