Seborrheic Keratosis
• Begin to appear during the 4th decade of life and then gradually increase in number.
• Macular, papular, or verrucous; colors vary from white to black but most commonly brown.
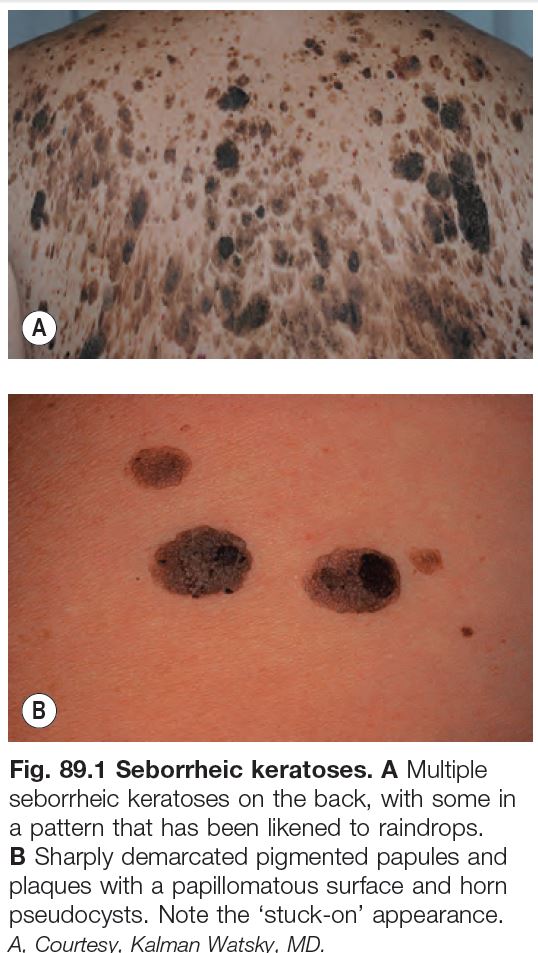
• Typically has a ‘stuck-on’ appearance with a smooth to verrucous surface (Fig. 89.1).
• Spares the palms, soles, and mucosal surfaces.
• May resemble a melanoma clinically but has no pigment network (by dermoscopy) and has horn pseudocysts.
• Sudden appearance of multiple lesions may be associated with internal malignancy (sign of Leser–Trélat) or erythroderma; the former may also be associated with skin tags, irritated seborrheic keratoses, tripe palms, and acanthosis nigricans.
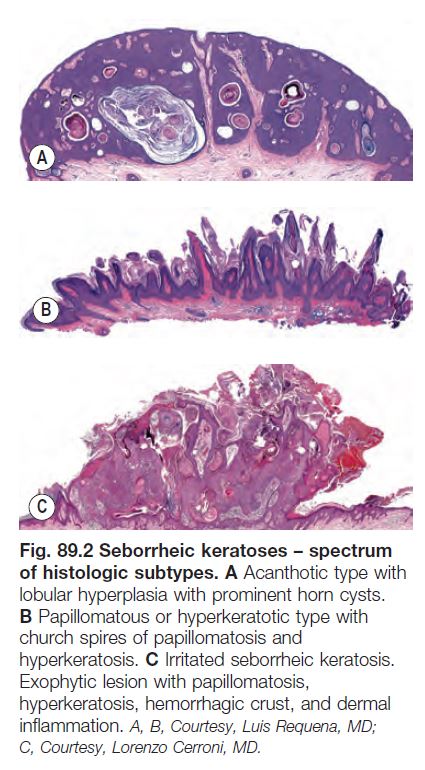
• Histopathology: a spectrum of different architectures, most commonly acanthotic, papillomatous and hyperkeratotic, or irritated (Fig. 89.2).
• Variants:
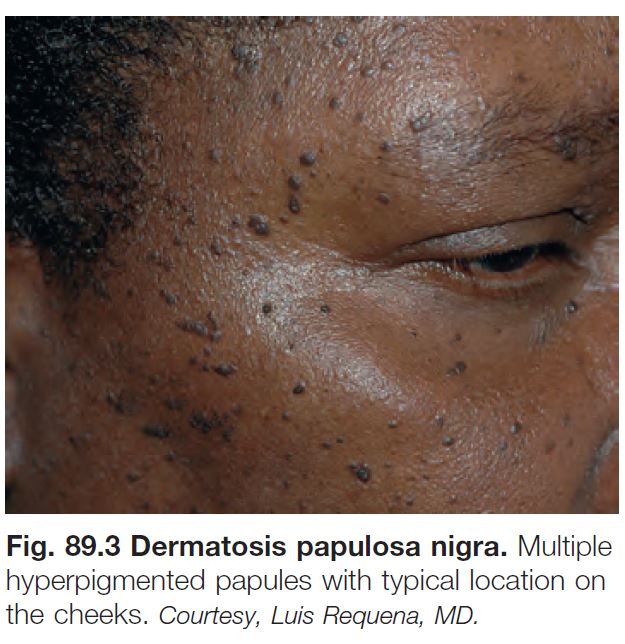
– Dermatosis papulosa nigra (Fig. 89.3): common in dark-skinned individuals; 1- to 5-mm hyperpigmented papules on the face.
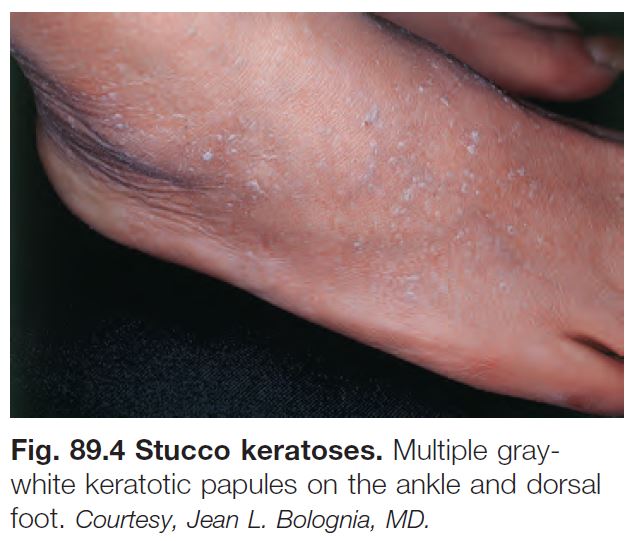
– Stucco keratosis (Fig. 89.4): 1- to 4-mm gray-white papules on the lower extremities (especially dorsal feet and ankles) of older adults.
– Inverted follicular keratosis: endophytic variant of seborrheic keratosis; tan to pink papule, typically on the face of adults.
Acrokeratosis Verruciformis
• Autosomal dominant disorder; sometimes associated with Darier disease.
• Multiple, skin-colored, flat-wart-like papules on dorsal aspect of hands and feet.
• Benign neoplasm of keratinocytes showing papillomatosis with overlying hyperkeratosis in ‘church spires’.
• May have ATP2A2 gene mutation.
Clear Cell Acanthoma
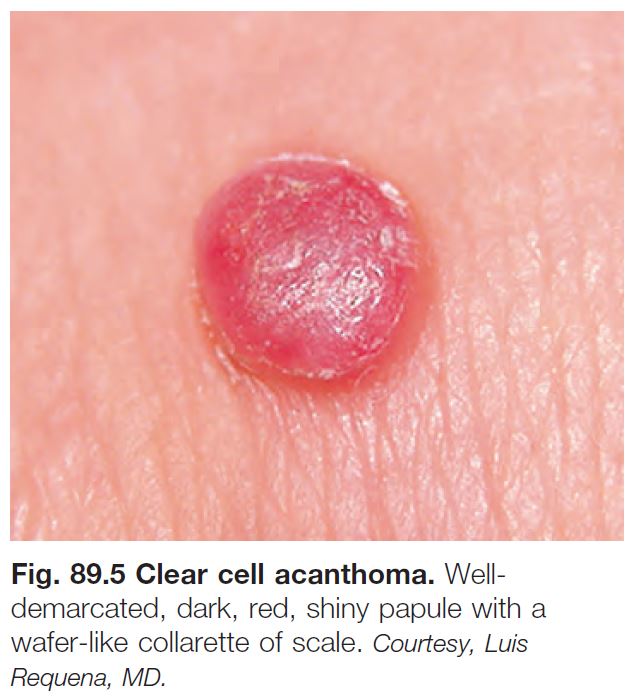
• Red, shiny papule or plaque, sometimes with a peripheral collarette of scale (Fig. 89.5).
• Favors the leg.
• Histopathology: acanthosis of characteristically well-demarcated pale or clear keratinocytes with overlying parakeratosis.
Large Cell Acanthoma
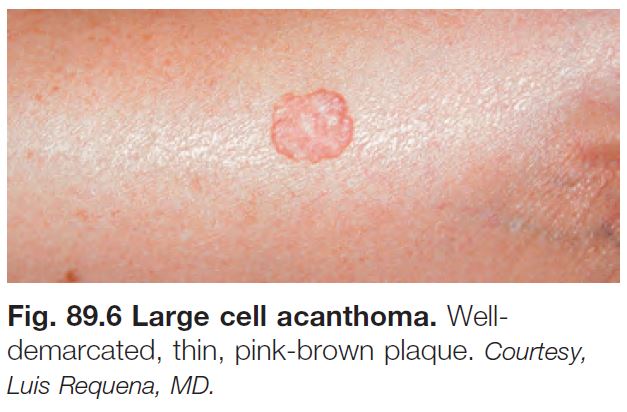
• Variably colored papule or plaque in sunexposed sites in older individuals (Fig. 89.6).
• A variant of actinic keratosis and seborrheic keratosis.
• Histopathology: orthokeratosis overlying a thin epidermis composed of enlarged keratinocytes.
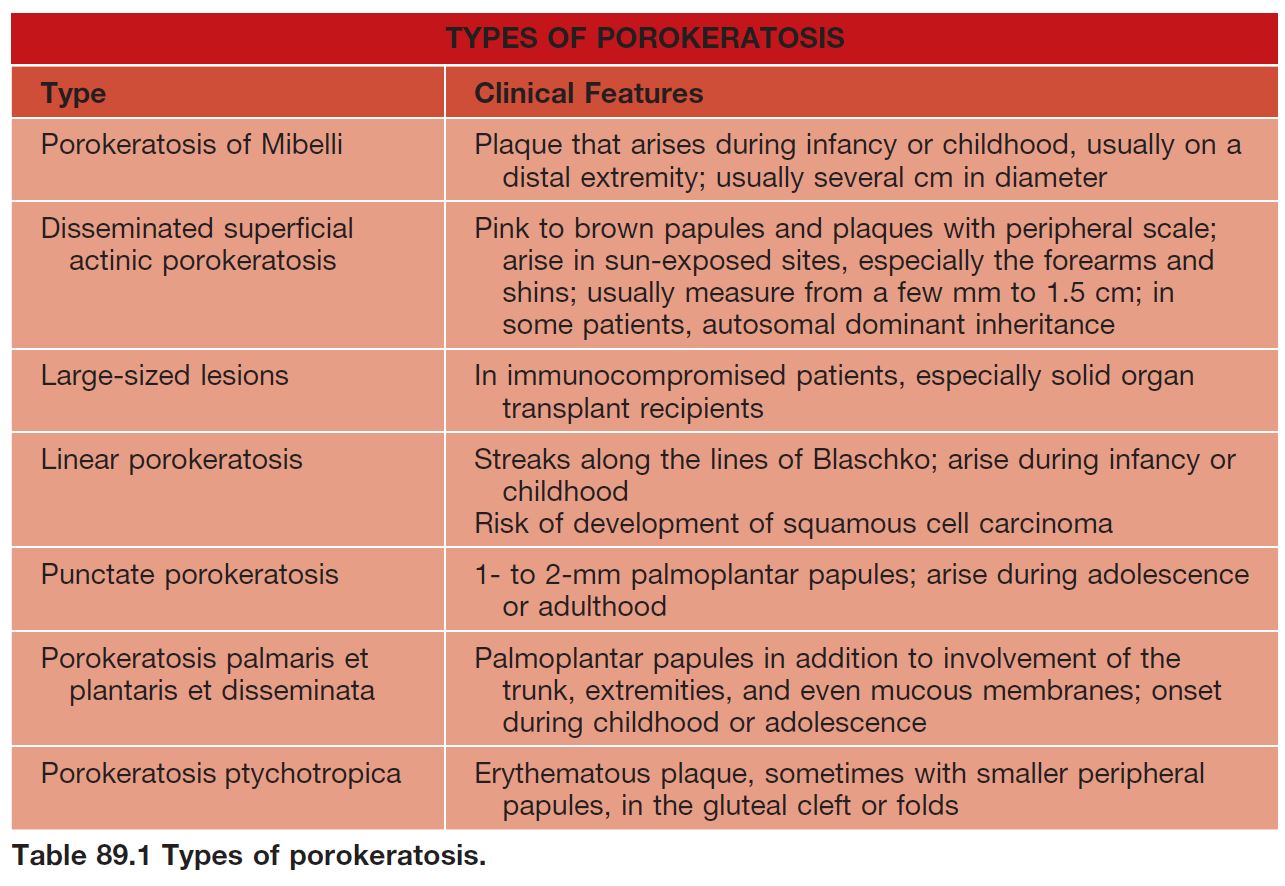
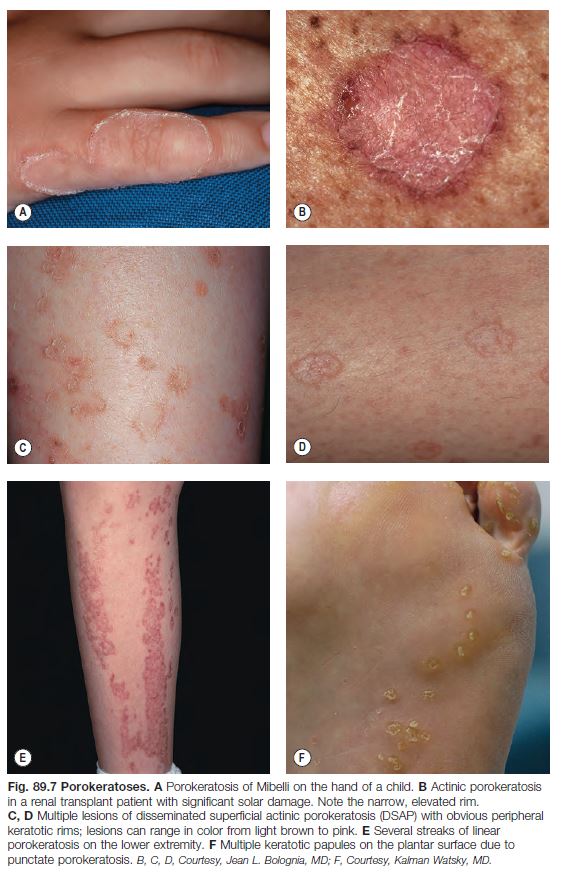
Porokeratosis
• Several different types (Table 89.1; Fig. 89.7).
• All have a distinctive thread-like border of scale that corresponds histopathologically to the cornoid lamella (column of parakeratosis histologically).
• The most common form, disseminated superficial actinic porokeratosis (DSAP), is sometimes misdiagnosed as multiple actinic keratoses.
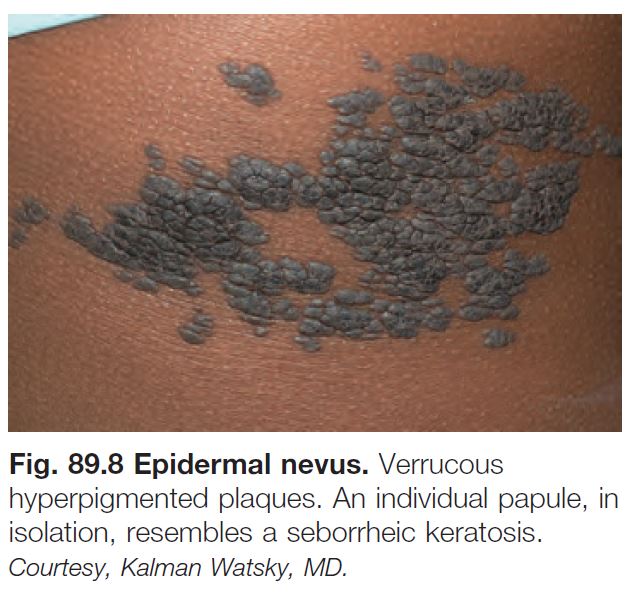
Epidermal Nevus (See Chapter 51)
• Hyperpigmented (rarely hypopigmented) papules and plaques (Fig. 89.8) along Blaschko’s lines.
• Verrucous, keratotic, velvety or barely elevated.
• May have a sebaceous or other adnexal component (i.e. nevus sebaceus), especially if on the scalp or face.
• Can be caused by mosaicism for mutations in FGFR3 (fibroblast growth factor receptor-3), PIK3CA, HRAS (also in nevus sebaceus), keratin 1 or 10 (if histologic finding of epidermolytic hyperkeratosis), and other genes.
• May be associated with extracutaneous manifestations (see Chapter 51).
Inflammatory Linear Verrucous Epidermal Nevus (See Chapter 51)
• Linear, pruritic, psoriasiform (erythematous with scale) plaques, usually on an extremity.
• 75% appear before age 5 years.
• DDx: primarily linear psoriasis (see Chapter 6).
Nevus Comedonicus
• Linear plaques composed of grouped comedones; may develop inflammatory acneiform lesions.
• 50% present at birth; otherwise, generally appear before age 10 years.
• May be due to mosaicism for a mutation in FGFR2.
Flegel’s Disease (Hyperkeratosis Lenticularis Perstans)
• Rare; may have an autosomal dominant inheritance.
• Onset usually during adulthood.
• Lentil-like keratotic papules on the distal lower extremities (Fig. 89.9).

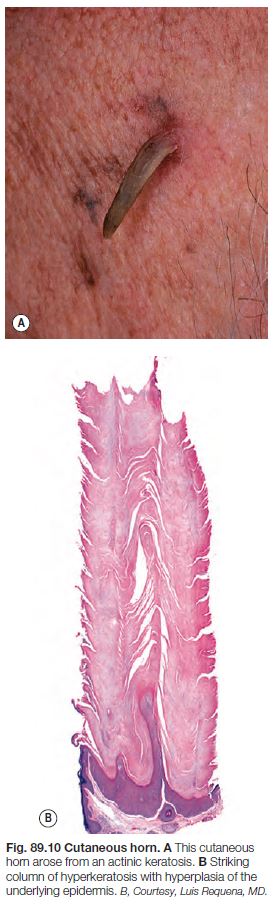
Cutaneous Horn
• Clinical term for marked hyperkeratosis arising from a papule or nodule (Fig. 89.10).
• The base of the lesion most commonly represents an actinic keratosis, seborrheic keratosis, verruca, or squamous cell carcinoma.
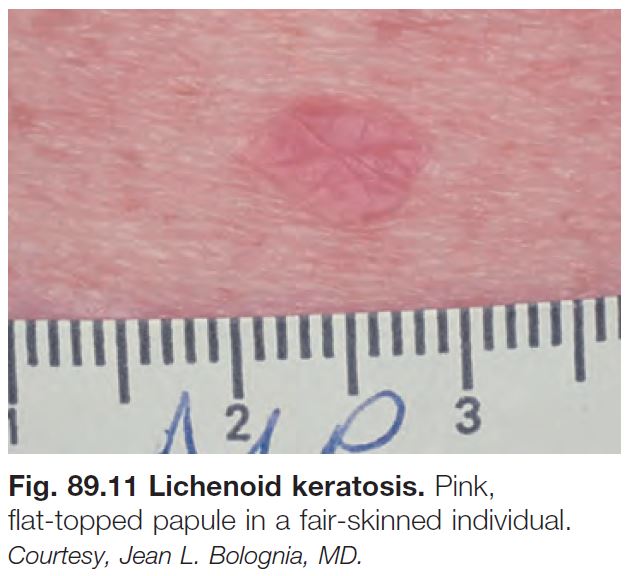
Solitary Lichenoid Keratosis/Lichen Planus-Like Keratosis
• Pink to pink-brown papule or plaque (Fig. 89.11); arises in chronically sun-damaged skin, most commonly on the chest, extensor upper extremities, and shins.
• Occasionally multiple.
• Clinically mimics an actinic keratosis and nonmelanoma skin cancer.
• Table 89.2 lists other solitary keratoses.
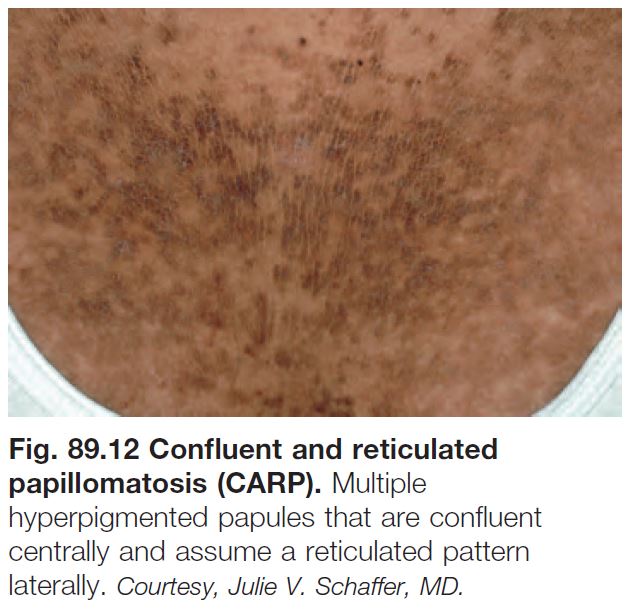
Confluent and Reticulated Papillomatosis (of Gougerot and Carteaud)
• Onset during puberty.
• Scaly to verrucous hyperpigmented plaques.
• Centrally confluent and reticulated at periphery (Fig. 89.12).
• Favors neck, central chest, submammary regions.
• Rx: oral tetracyclines (e.g. minocycline).