Introduction
• Adipose tissue plays many active roles in the body beyond insulation, e.g. storing and releasing lipids, mediating inflammation, and modulating endocrinologic and reproductive systems.
• Panniculitis = inflammation of adipose tissue.
• Clinically and histopathologically, the adipose tissue has a limited repertoire of responses to insults and inflammation.
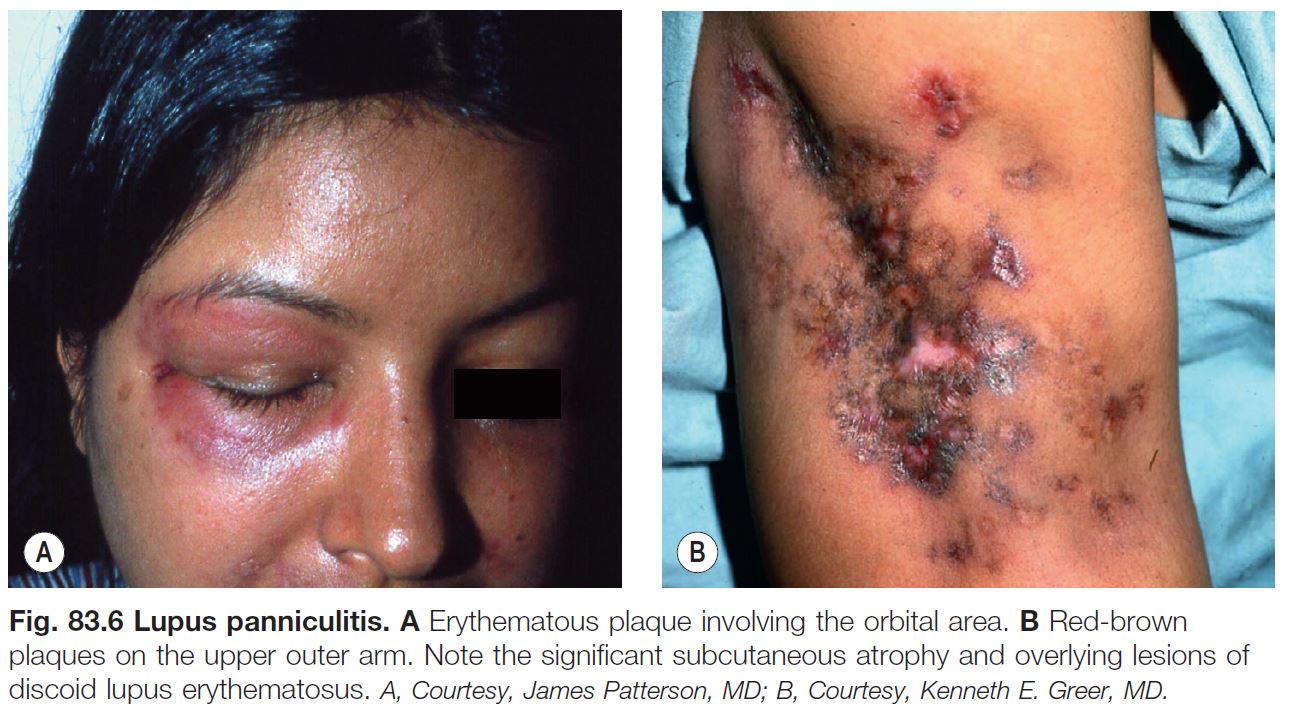
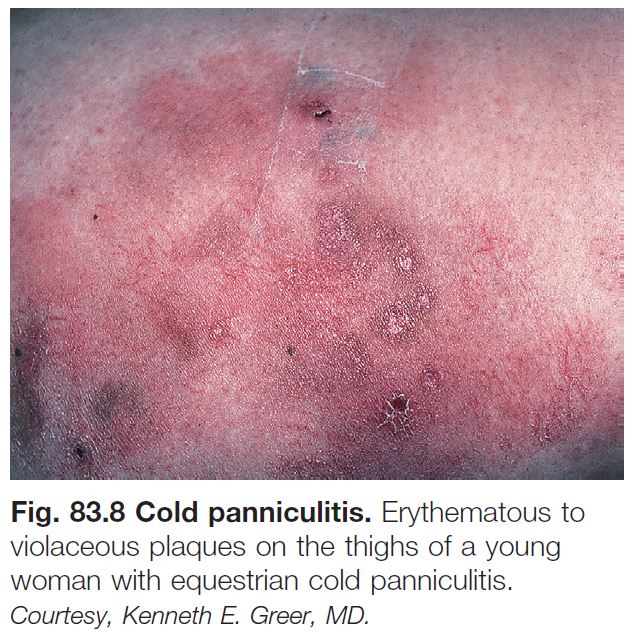
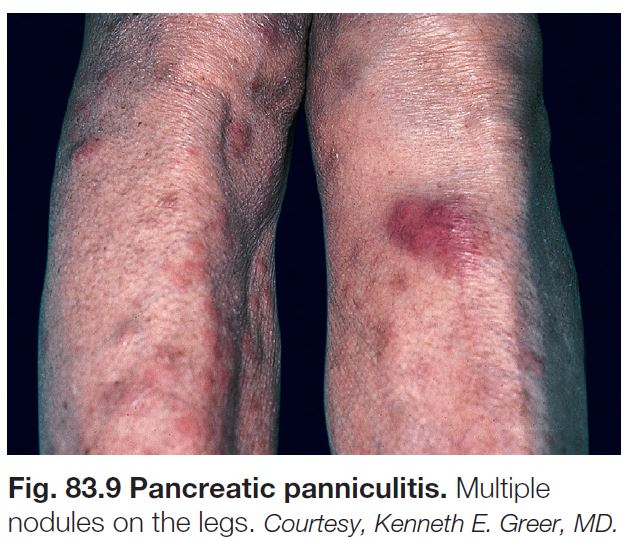
• Most often clinically presents as tender, inflamed, subcutaneous nodules or plaques; with the exception of erythema nodosum, ulceration with drainage may develop.
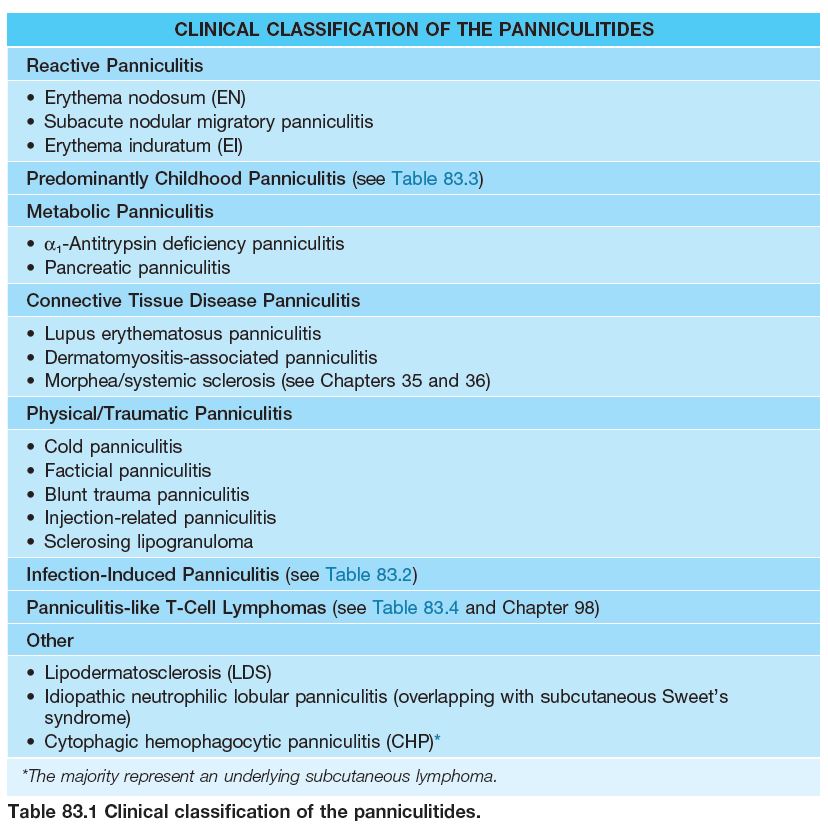
• There are various etiologies, and a clinical classification system is presented in Table 83.1.
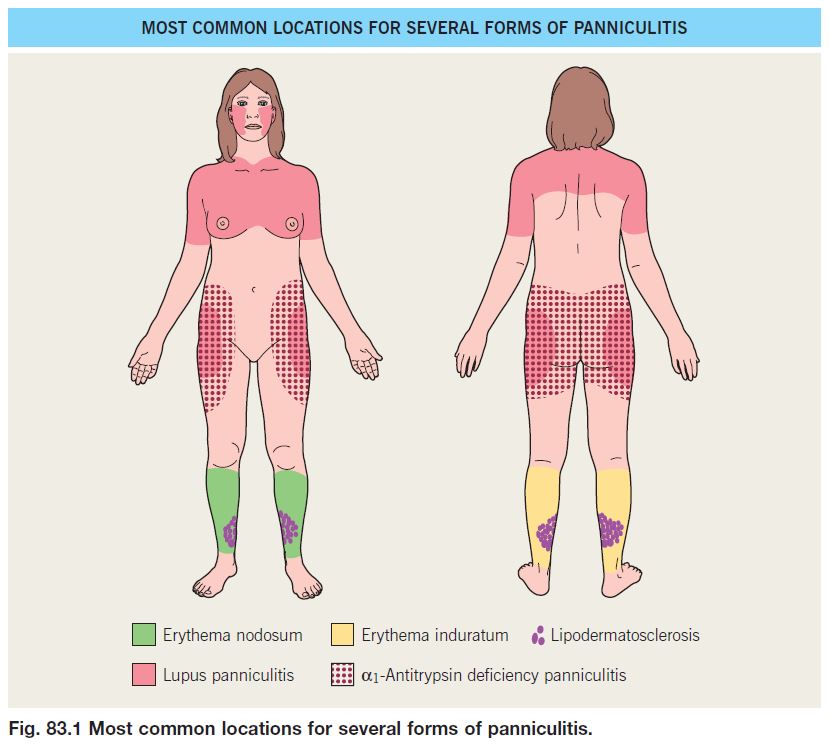
• Diagnosis is challenging and involves consideration of (1) patient characteristics such as age, immune status, underlying diseases; (2) location of the lesions (Fig. 83.1); (3) the presence or absence of ulceration and/or drainage; and (4) histopathological findings.
• A biopsy is usually necessary to establish the diagnosis, and it is critical that the specimen include a generous portion of the subcutaneous (SC) fat.
• Excisional biopsies or narrow incisional biopsies that incorporate a broad expanse of SC fat are preferable to punch biopsies.
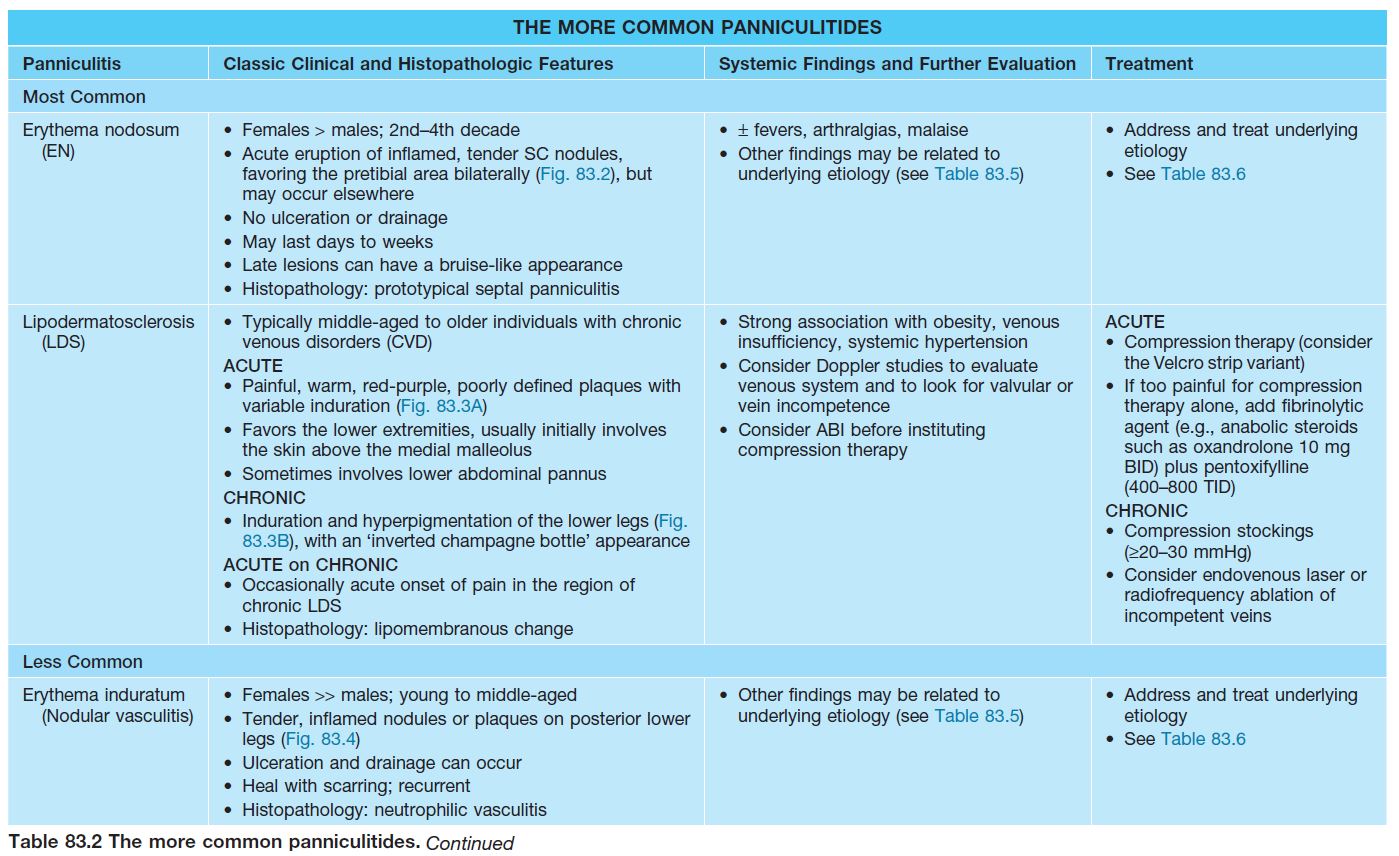
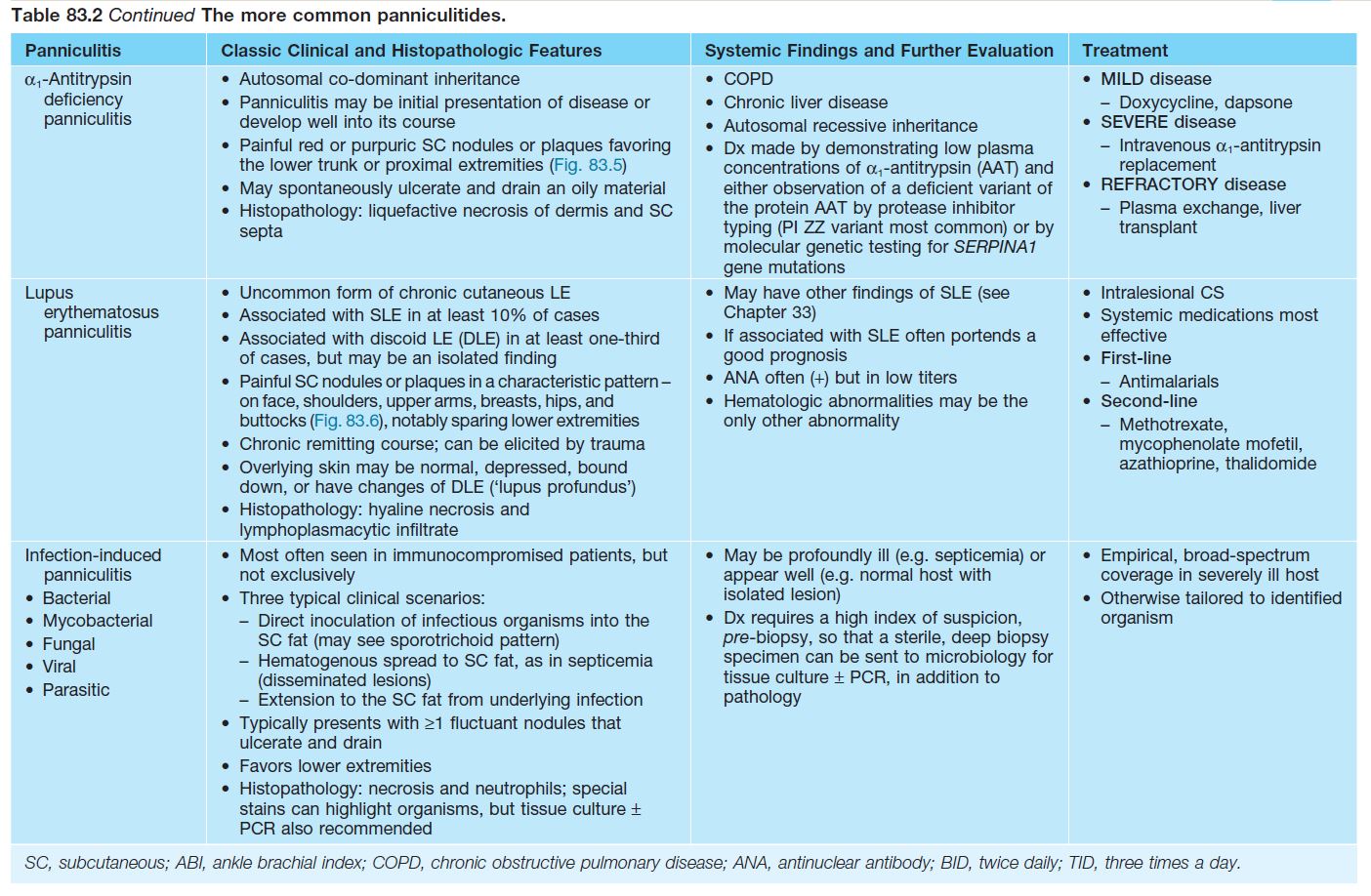
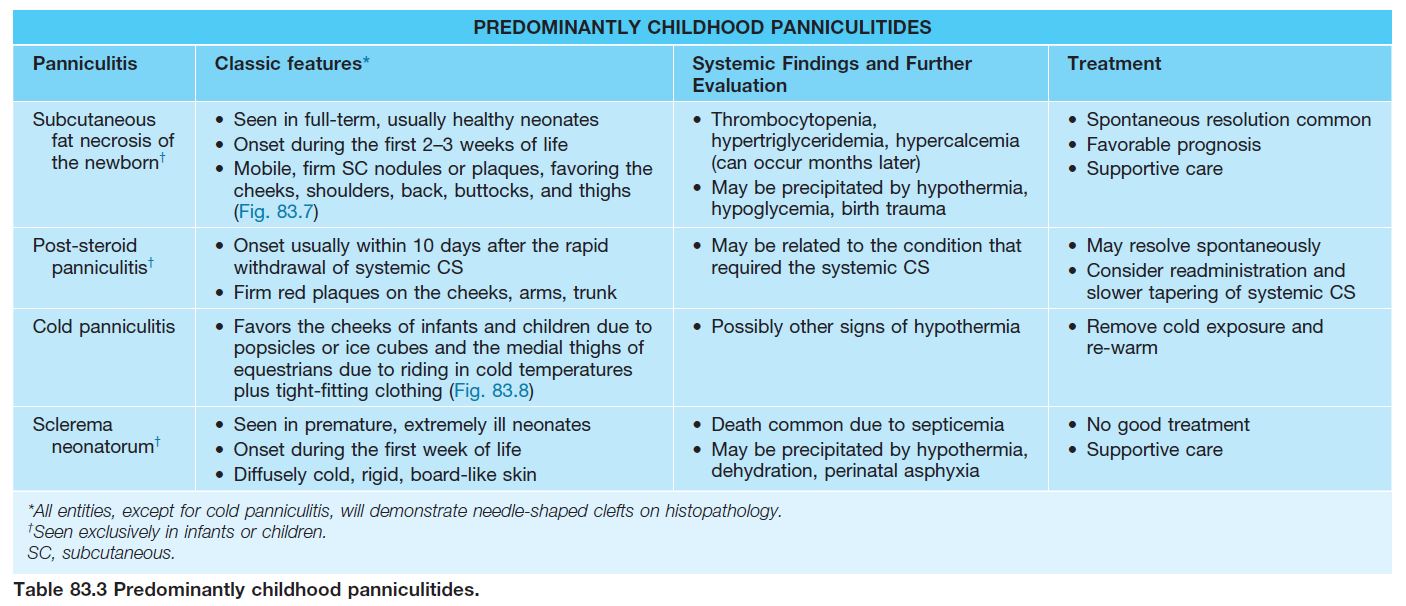
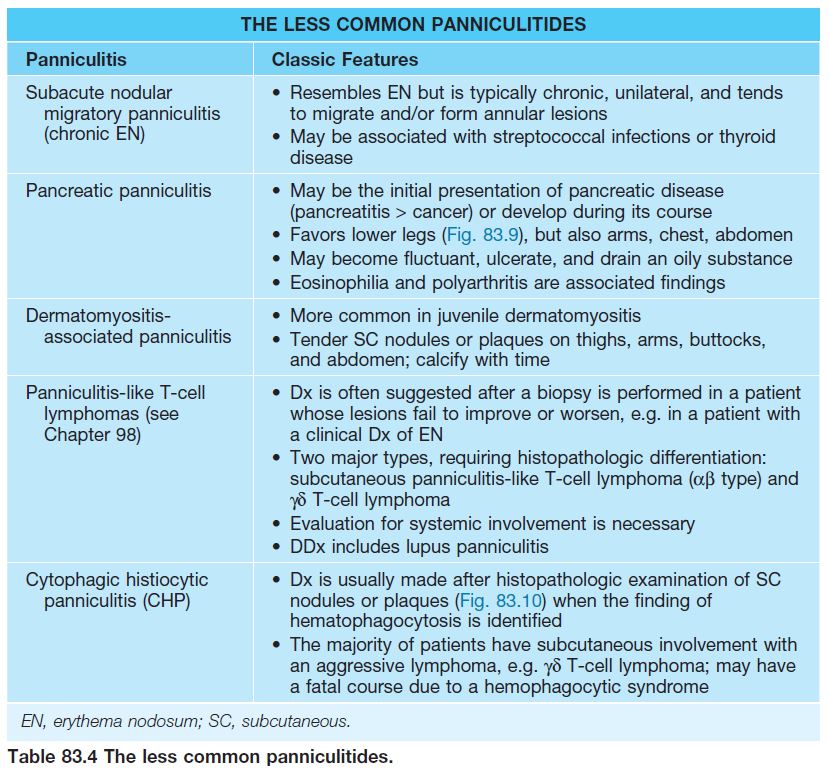
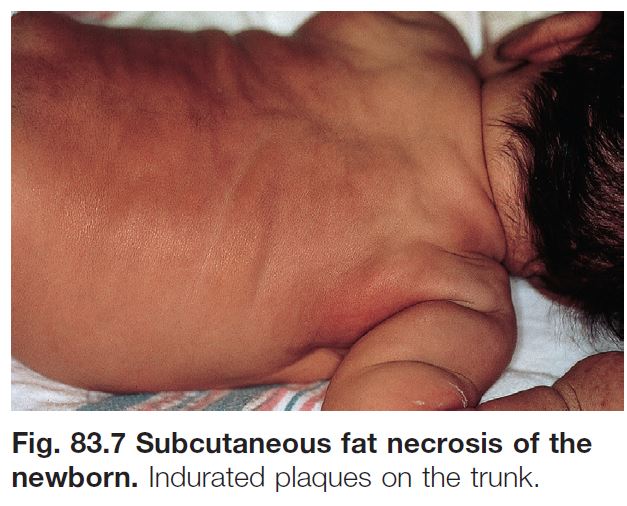
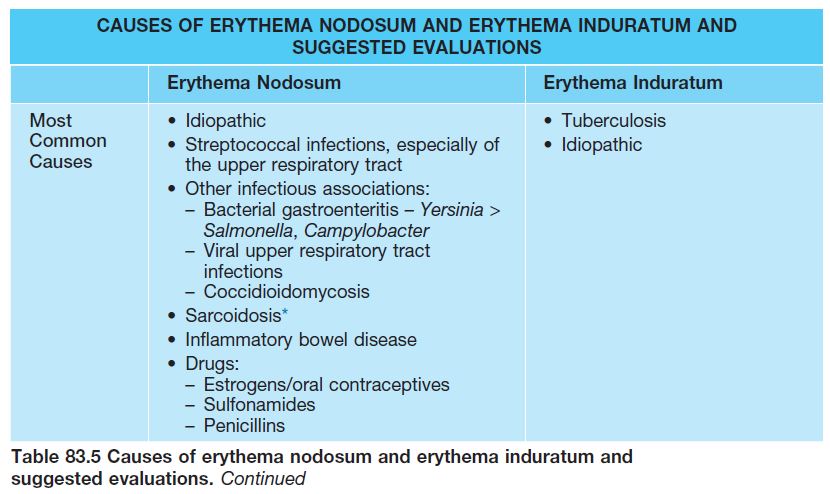
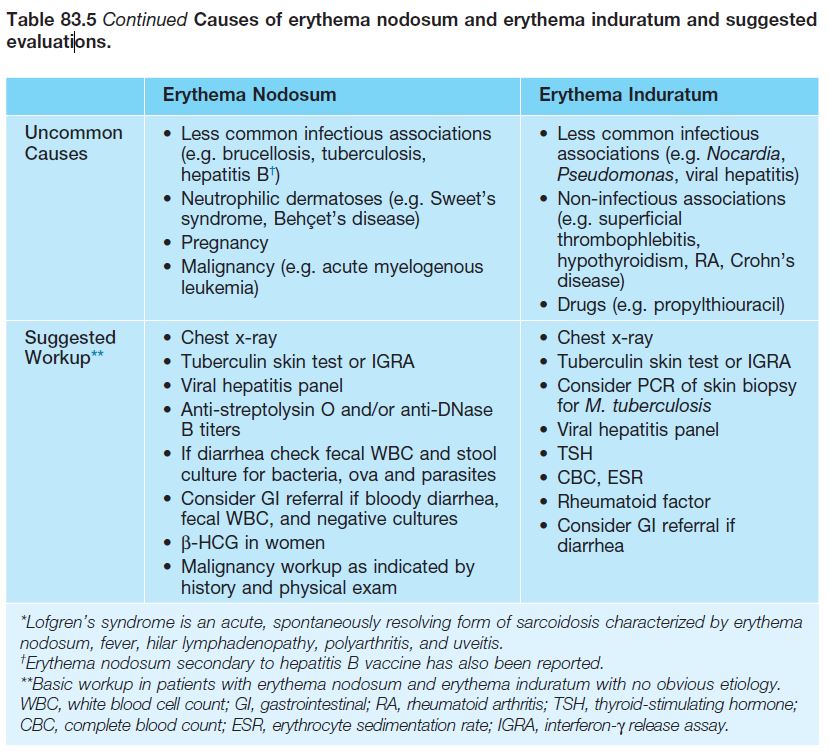
• Once the diagnosis of panniculitis is made, further evaluation for underlying etiology or associated conditions is necessary (Tables 83.2–83.4).
• DDx: Primarily differentiating among the various forms of panniculitis, superficial thrombophlebitis.
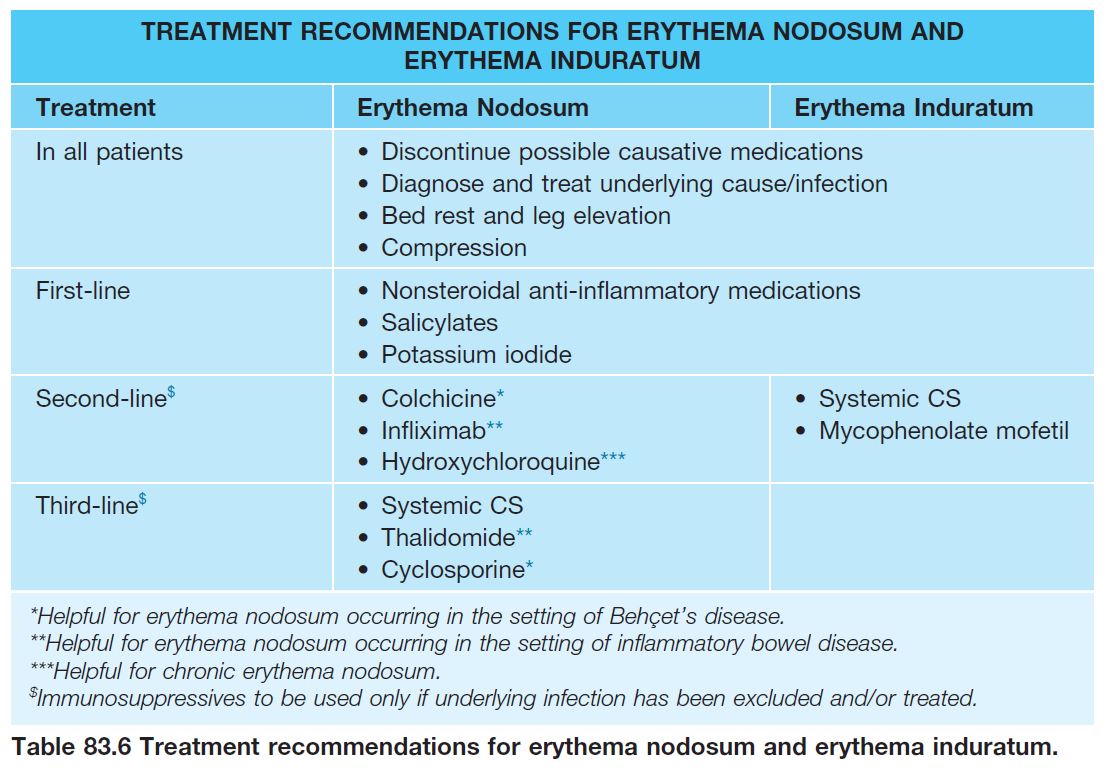
• Rx: involves specific treatment of the panniculitis and often treatment of an underlying disorder (see Tables 83.2–83.4).