Key Points
• Cutaneous xanthomas are due to an accumulation of lipid, primarily within dermal macrophages (foam cells), and they have a characteristic yellow-orange hue.
• Four major types of xanthomas: eruptive, tuberous, tendinous, and plane.
• They may be a sign of hyperlipidemia, either primary or secondary, or an underlying monoclonal gammopathy.
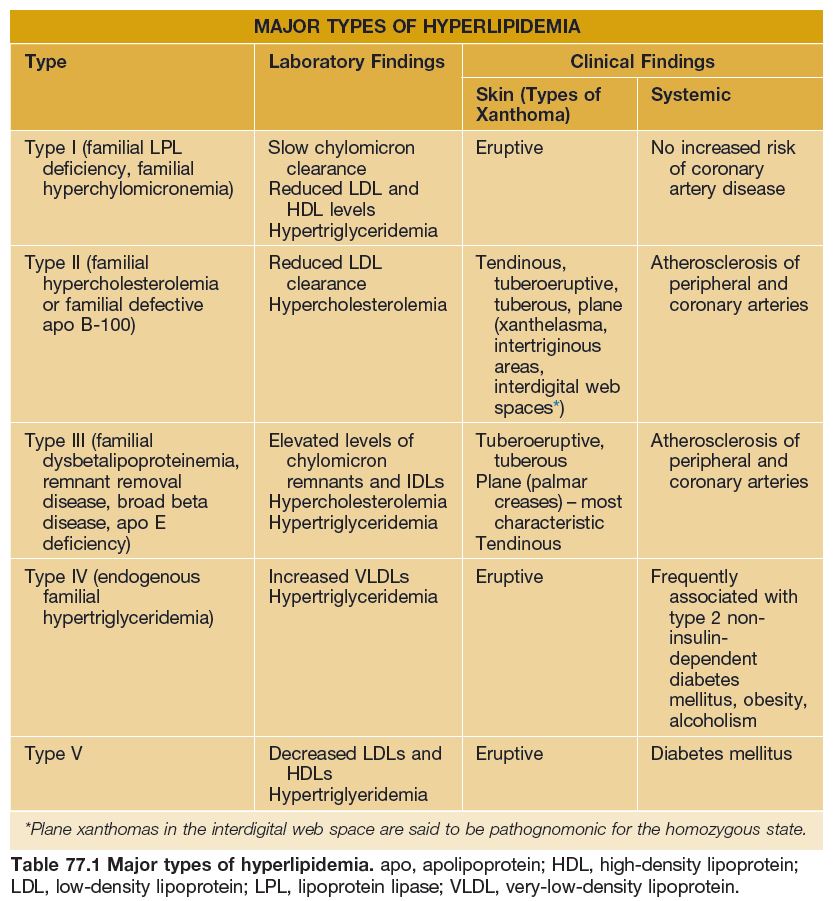
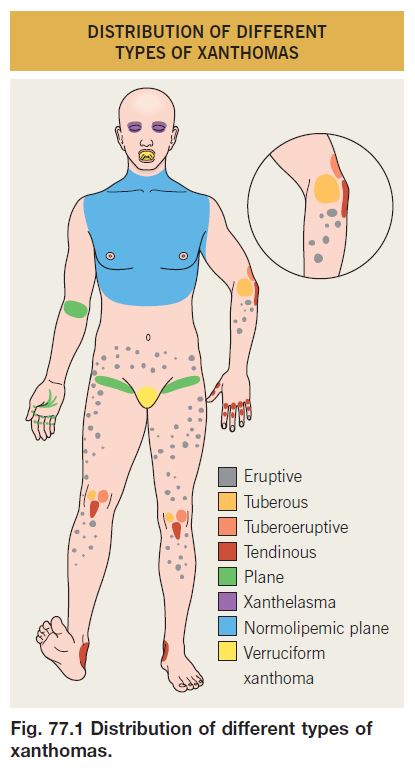
• The type of xanthoma and its anatomic location are clues to the specific lipid abnormality or associated disorder (Table 77.1; Figs. 77.1 and 77.2).
• DDx depends on the type of xanthoma (Table 77.2).
• In general, Rx is focused on correcting any underlying hyperlipidemia.

Xanthomas Associated with Hyperlipidemia
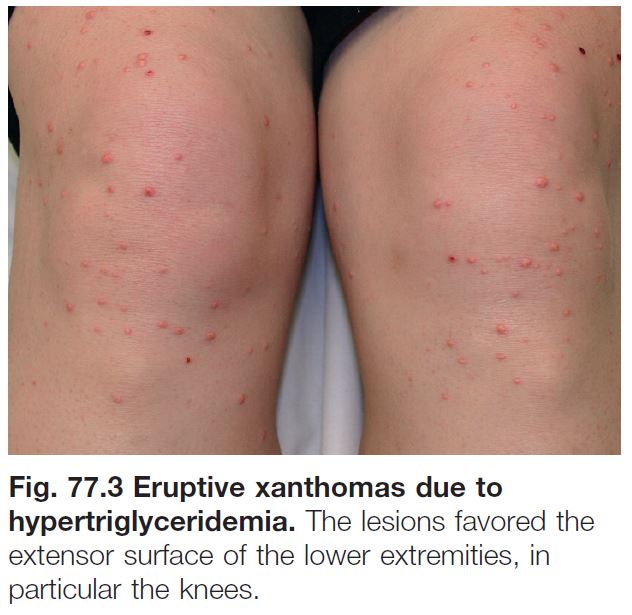
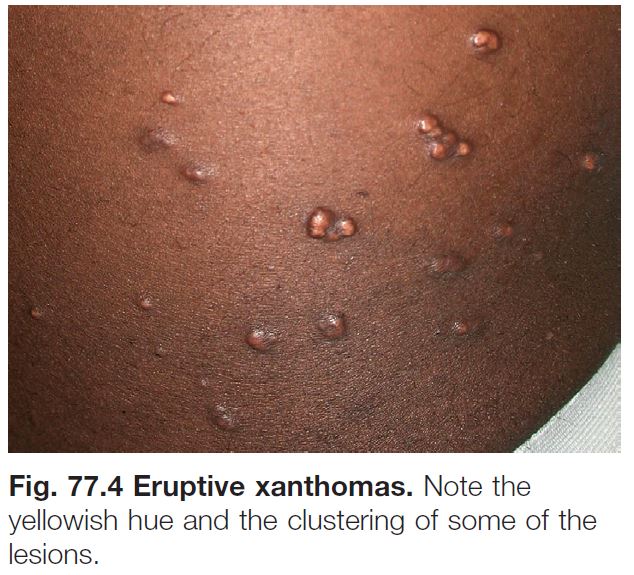
Eruptive Xanthomas
• Yellow-pink papules, 1–5 mm in diameter.
• May be widespread, but favor the extensor surfaces of the extremities and buttocks (Figs. 77.3 and 77.4).
• An inflammatory halo, tenderness, and/or pruritus may be present.
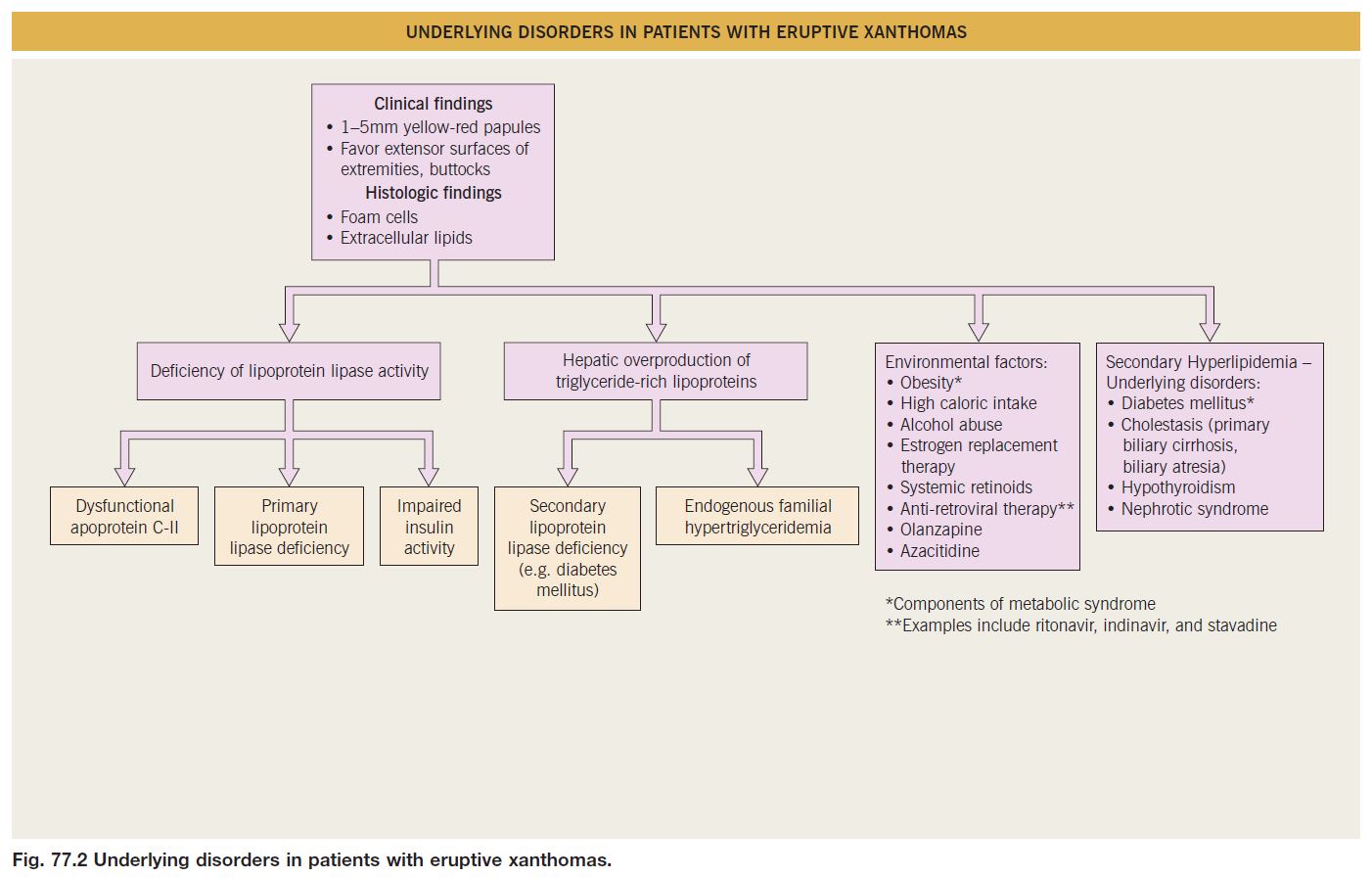
• Associated with hypertriglyceridemia (often >3000–4000 mg/dl) (see Fig. 77.2).
• Seen in the setting of type I, IV, or V hyperlipidemia and most commonly when associated diabetes mellitus is under poor control.
• Lesions often resolve within weeks of aggressive Rx: insulin; triglyceride-lowering agents, e.g. fenofibrate.
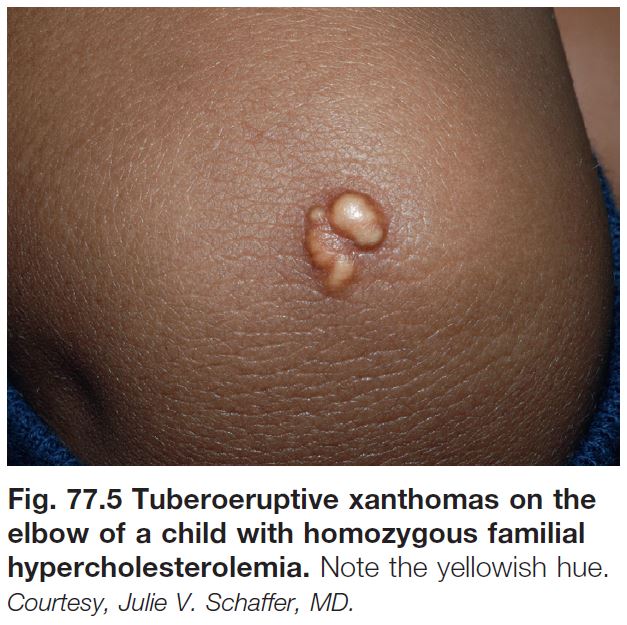
Tuberous/Tuberoeruptive Xanthomas
• Pink-yellow to yellow-brown papules (tuberoeruptive) or nodules (tuberous) on extensor surfaces, especially the elbows and knees (Figs. 77.5 and 77.6); tuberous xanthomas can be >3 cm in diameter.
• Associated with hypercholesterolemia (type II or III hyperlipidemia).
• May be slow to regress with cholesterollowering agents (e.g. ‘statins’).

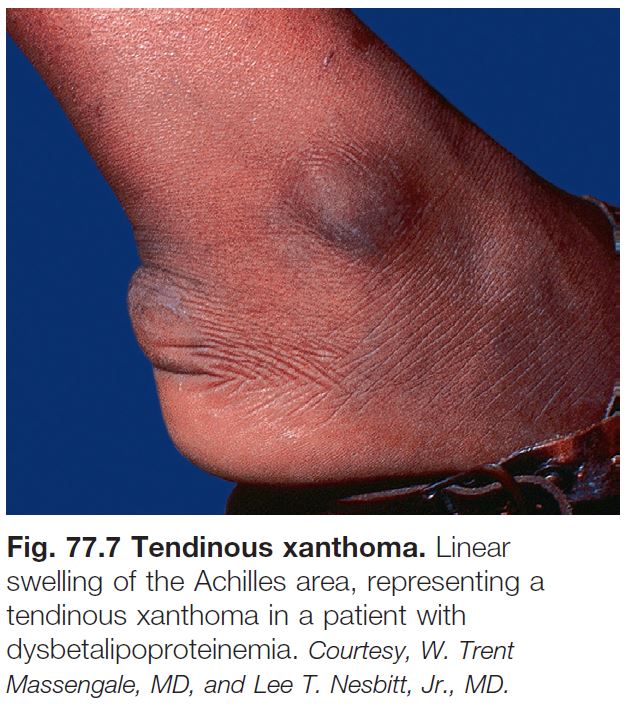
Tendinous Xanthomas
• Firm, smooth, skin-colored nodules due to lipid deposits within the Achilles tendons and the extensor tendons of the hands, knees, and/or elbows (Figs. 77.7 and 77.8).
• Can serve as an early clue to the presence of type II hyperlipidemia.
• Rarely form as a consequence of accumulation of cholestanol (cerebrotendinous xanthomatosis) or plant sterols (β-sitosterolemia).

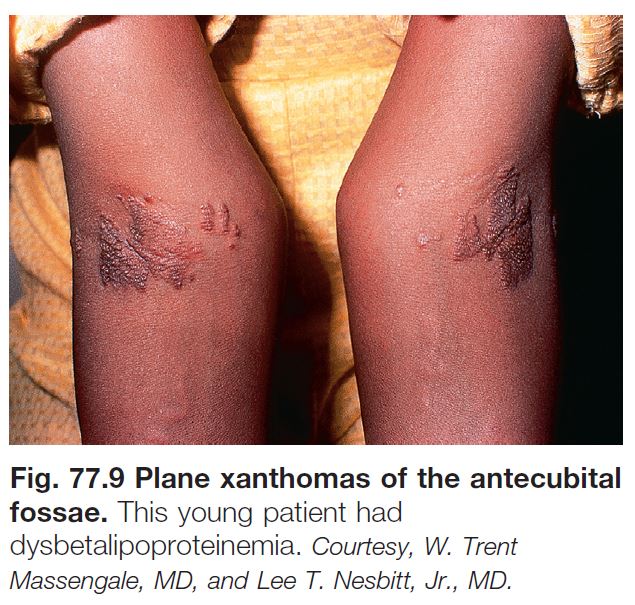
Plane Xanthomas and Xanthelasma
• Yellow to orange macules and patches or thin papules and plaques.
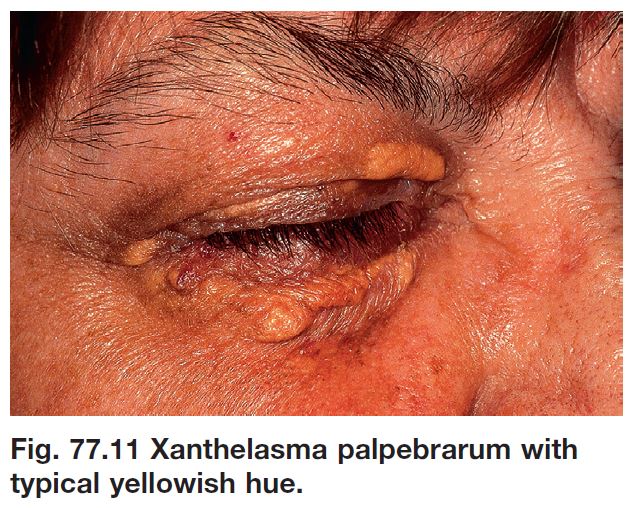
• Of the different types of xanthomas, xanthelasma is the most common; however, hyperlipidemia is detected in only 50% of patients.
• Site:
– Intertriginous – antecubital fossae, finger web spaces, and palmar creases (Figs. 77.9 and 77.10).
– Eyelids (xanthelasma), especially the medial aspect of the upper eyelid (Fig. 77.11).
• Intertriginous plane xanthomas can be seen in primary hyperlipidemia (type II or III) as well as secondary hyperlipidemia (e.g. biliary atresia, primary biliary cirrhosis).
• Rx of xanthelasma: destructive methods (e.g. trichloroacetic acid application, laser ablation), surgical excision.
Laboratory evaluation for suspected hyperlipidemia is outlined in Table 77.3.

Normolipemic Xanthomas
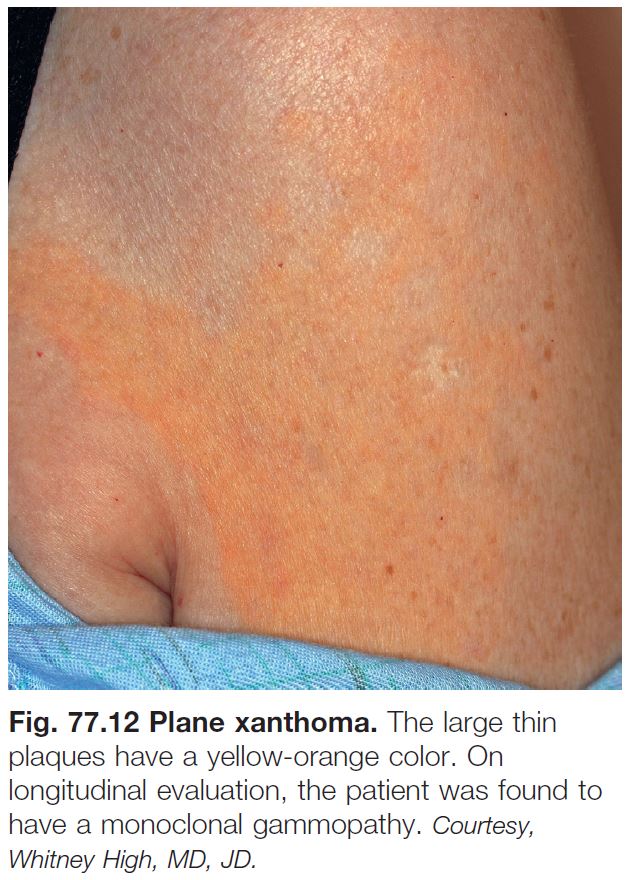
Plane Xanthomas Associated with Monoclonal Gammopathy
• In contrast to plane xanthomas due to hyperlipidemia, these yellow-orange patches and thin plaques are usually larger in size and have a more extensive distribution pattern; the latter often includes the trunk (Fig. 77.12).
• In addition to the trunk, lesions may be seen on the neck, in flexural folds, and in the periorbital region.
• The monoclonal gammopathy is most commonly due to a plasma cell dyscrasia, and occasionally due to a lymphoproliferative disorder.
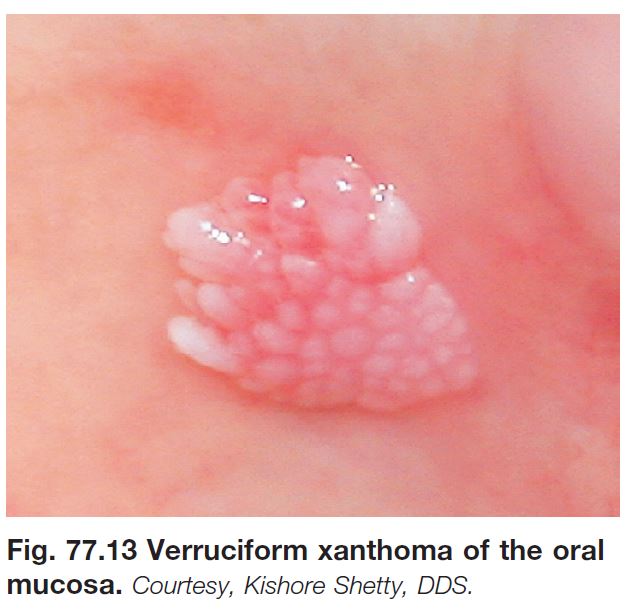
Verruciform Xanthoma
• Asymptomatic verrucous plaque, 1 to 2 cm in diameter (Fig. 77.13).
• Oral mucosa or anogenital region.
• May be seen in association with lymphedema, epidermolysis bullosa, and CHILD (congenital hemidysplasia with ichthyosiform erythroderma and limb defects) syndrome.