Trigeminal neuralgia is characterised by recurrent brief episodes of one-sided electric shock-like pains, sudden onset and termination, in the distribution of one or more divisions of the trigeminal nerve that are typically triggered by light touch on face. Trigeminal neuralgia is a rare condition that affects women more than men. Trigeminal neuralgia is commonly seen more in the older adult population. The incidence increases gradually with age; most idiopathic cases begin after the age 50, although onset may occur in the second or third decades or, rarely, in children.
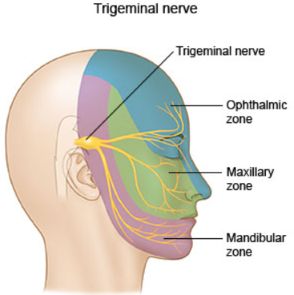
The trigeminal nerve is the 5th cranial nerve. It is the sensory supply to the face and the sensory and motor supply to the muscles of mastication (chewing). It has three major divisions:
- Ophthalmic (V1)
- Maxillary (V2)
- Mandibular (V3)
The nerve starts at the midlateral surface of the pons, and its sensory ganglion resides in Meckel's cave in the floor of the middle cranial fossa.
Most common cause of trigeminal neuralgia is caused by compression of the trigeminal nerve root, usually within a few millimeters of entry into the pons. Compression by an artery or vein is thought to account for 80 to 90 percent of cases. Other causes of trigeminal nerve compression can be caused by vestibular schwannoma (acoustic neuroma), meningioma, epidermoid or other cyst, rarely, a saccular aneursym or arteriovenous malformation. The compression of the nerve leads to demyelination of the nerve causing the pain.
Trigeminal neuralgia is diagnosed clinically. Criteria for trigeminal neuralgia are as follows:
- A) At least three attacks of unilateral pain fullfilling criteria B and C
- B) Occurring in one or more divisions of the trigeminal nerve, with no radiation beyond the trigeminal distribution
- C) Pain has at least three of the following four characteristics:
- Recurring in paroxsymal attacks lasting from a fraction of a second to two minutes
- Severe intensity
- Electric shock-like, shooting, stabbing, or sharp in quality
- At least three attack triggered by light touch to the affected side of the face
- D) No clinically evident of neurological deficit
- E) Not better accounted by any other diagnosis
MRI of brain is useful to rule out any abnormalities such as compression of trigeminal nerve by artery, vein, cyst and tumour.
Management:
- Pain due to trigeminal neuralgia can be managed with medications such as cabarmazepine. However, it has side effects causing drowsiness, dizziness and nausea.
- Oxcarbazepine can also be used to manage the pain.
- Lamotrigine is another alternative if patient does not respond well to cabarmazepine or oxcarbazepine. However, it is not covered under PBS for this indication and patient will have to pay full price for the medication.
- Botox injection may be beneficial in patient not getting relief with medication. No strong evidence on the research for the use of Botox injection at this stage. Botox injection can also be very costly and can only be done by trained doctors.
- Surgery involves microvascular decompression with craniotomy and the removal or separation of blood vessels away from trigeminal nerve (if there is compression of trigeminal nerve root) to relieve the pain. The surgery does carry risk of cerebrospinal fluid leak, infarction or blood clot.
- Rhizotomy is a procedure used to ablate the trigeminal ganglion or root. This procedure carry risk of meningitis, loss of sensation on face and corneal ulcer.
- Radiosurgery involves ablating the trigeminal nerve root or ganglion using focussed gamma radiation. Again, it can cause loss of sensation on face.